A sentinel lymph node is the first node or nodes in the armpit that receive the lymphatic drainage from the breast. If cancer exists in the breast, it might escape to the armpit lymph nodes via these breast lymphatics. Therefore, whenever women have an operation for invasive breast cancer, surgeons routinely check the armpit to see if cancer has spread to the lymph nodes. This is called a sentinel lymph node biopsy.
 We’ve been working hard on this. Add your e-mail address and we will tell you as soon as it launches.
We’ve been working hard on this. Add your e-mail address and we will tell you as soon as it launches.How is it Done?
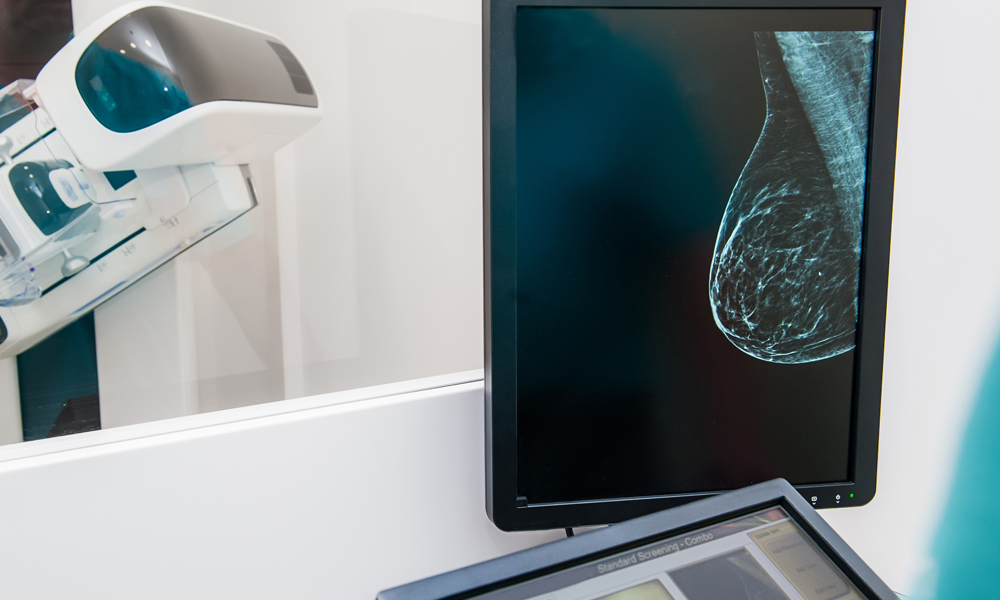
Identification of the sentinel lymph node(s) is accomplished by injecting blue dye, radioactive tracer, or both, into the breast prior to lumpectomy or mastectomy. The dye and/or tracer then travel into the armpit, and turn an average of two nodes bright blue, or radioactive when using tracer. The blue or radioactive nodes are the sentinel nodes. These get removed via a small incision in the armpit and are thoroughly tested by a pathologist. This analysis will reveal whether or not cancer has spread from the breast to the lymph nodes.
If cancer has not spread, the nodes are “negative”, indicating early stage breast cancer. If cancer has spread to the nodes, the nodes are called “positive”, and additional treatments must be considered: further surgery, radiation, and chemotherapy. In response to an exciting discovery published in 2011 by Dr. Armando Giuliano, et.al., many surgeons no longer remove additional armpit lymph nodes even after cancer is found in the sentinel nodes. We now recommend only radiating the remaining nodes (in most cases) because no significant difference was found in overall survival or nodal recurrence rates when leaving the rest of the nodes.[i]
Prior to the era of sentinel lymph node biopsy, surgeons would remove all of the armpit lymph nodes to make sure the cancer did not spread. This procedure, called a complete axillary node dissection, resulted in complications in up to 84% of patients, including pain, numbness, arm swelling (lymphedema), fluid buildup (seroma), limited arm movement, and infection.[ii] [iii] [iv] On the other hand, sentinel lymph node biopsy reduces these complications to under 10%.[v] [vi]